“Pharmaceutical grade” is the phrase every grey-market vendor reaches for, and almost nobody who uses it has read what pharmaceutical grade actually requires. We did. Then we measured 62,079 independent peptide certificates against the real rules. This is the dated, source-linked record of how far apart the two worlds are, and where the gap is not where you would guess. All corpus figures below are as of July 31, 2026.
- Pharma's dose bar is ±10%, not perfection, and only about half the grey market clears it. A USP-compliant 100mg tablet can measure 90mg to 110mg and pass. Across 40,271 grey-market certs with a usable dose figure, 51.3% land inside that same ±10% bar (median miss 9.7%), and the median product is over-filled by 7.35%. That is a bare majority, not a comfortable one. The tails are worse: 680 certs are underfilled by 40% or more.
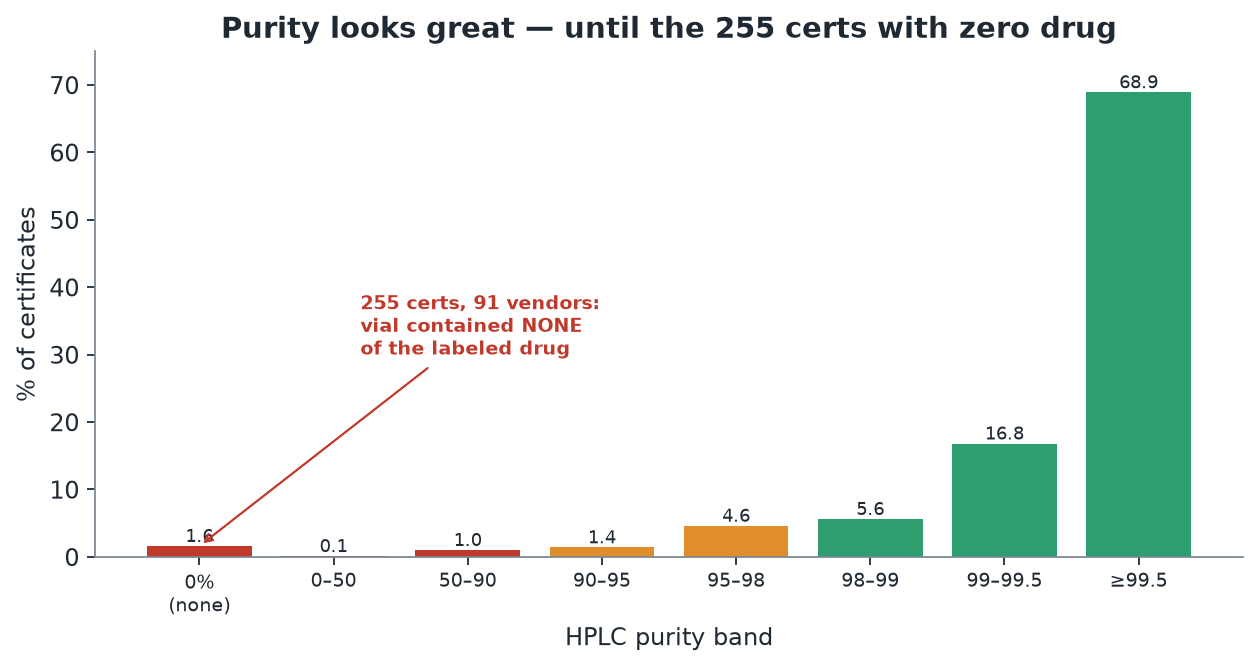
- Purity is a decoy. Median grey-market purity is 99.73%, and that number sells a lot of vials. But purity for peptides is allowed to run far looser than people think (peptides are explicitly carved out of the small-molecule impurity rules), and worse, 269 certificates across 95 vendors reported 0% of the labeled drug, the literal "sample does not contain" result. A vial can read 99% pure and still hold a fifth of the dose, or none of the molecule.
- The endotoxin gap is the real story. Every pharmaceutical injectable lot is tested for bacterial endotoxin (USP <85>) because a perfectly sterile vial can still cause septic shock. In our corpus, only 7.5% of certs report an endotoxin result at all. Among the few that do, about 1 in 88 fails. The pharma bar (every lot tested and passing) is met by 7.4% of the corpus.
- Pharma fails too, and that is the point. Real 2023 to 2026 recalls include IV bags at twice the labeled dose and a compounded semaglutide at 79.9% potency. The difference is not that pharma never errs. It is that a system catches the error and recalls the lot. The grey market has no such system, and it publishes its passing tests while the failures stay in private chats.
- First, the rules pharma actually follows
- Dose: a 20-point-wide bar, and where the vials land
- Purity: the number everyone screenshots, and the vials with nothing in them
- Endotoxin: the test pharma never skips, and grey market never runs
- What pharma has that grey market doesn’t: a system
- How this scores every vendor on this site
- What a buyer should take from this
First, the rules pharma actually follows
Start with the number that surprises people: a pharmaceutical tablet does not have to contain exactly what its label says. The standard USP monograph assay window is 90.0% to 110.0% of the labeled amount. Acetaminophen tablets: not less than 90.0%, not more than 110.0%. Ibuprofen: the same. The tolerance is written into the USP General Notices, which state plainly that the limits “allow for analytical error, for unavoidable variations in manufacturing and compounding, and for deterioration to an extent considered acceptable under practical conditions.” A 100mg tablet that assays at 92mg is not defective. It is compliant.
Some drugs are held tighter. Metformin runs 95.0% to 105.0%. Levothyroxine, a thyroid drug with a narrow therapeutic window, was narrowed by the FDA in 2007 from 90 to 110 down to 95 to 105 across its entire shelf life, and it took a federal action to impose even that. The takeaway is not that pharma is sloppy. It is that the industry that wrote the rulebook decided a few percent off label is the realistic, safe, achievable standard for a regulated factory. Anyone promising you a hand-mixed vial is dead-on 100% is selling a fantasy the pharmaceutical industry never promised itself.
Two more pharma facts matter for what follows, because the grey market gets both wrong in its marketing.
Purity. “95% pure, therefore garbage” is a myth. The international impurity rules that push small molecules to very high purity, ICH Q3A, explicitly exclude peptides in their first paragraph. Peptides are hard to purify because their impurities are closely related sequences, deletions and truncations that co-elute with the target, so peptide specifications run looser impurity allowances by design. A peptide active ingredient can be in the mid-90s on a purity assay and still be a compliant, properly specified product, if there is a specification, a monograph, and released test data behind it. Hold that conditional. It is the whole game.
Endotoxin. This is the one pharma never bends on. Bacterial endotoxin is lipopolysaccharide shed from the cell walls of gram-negative bacteria, and it causes fever, septic shock, and organ failure at nanogram levels. The critical, counterintuitive fact: endotoxin survives autoclaving. Standard 121C steam sterilization kills bacteria but leaves their endotoxin intact; destroying it takes dry heat at around 250C. So a vial can be perfectly sterile and still pyrogenic. That is why USP <85> sets a hard endotoxin limit (the formula is K divided by M, with K = 5 endotoxin units per kilogram for a normal injection, which works out to a ceiling of about 350 endotoxin units for a 70kg adult), and why every injectable lot is tested for it before release. It is not optional, and it is not skippable.
And pharma still fails. A compounding pharmacy recalled IV bags that may have held twice the labeled dose. A compounded semaglutide was found at 79.9% potency. Subpotent levothyroxine has been recalled more than once. The honest comparison is not pharma-perfect versus grey-market-bad. It is a system that tests every lot and recalls the failures, against a market that has no required testing at all. Keep that frame. Now the measurement.
Dose: a 20-point-wide bar, and where the vials land
We pulled every published certificate in our corpus carrying a usable dose-versus-label figure, 40,271 of them as of July 31, 2026. The bar is the pharmaceutical one: within 10% of label is the assay tolerance, within 15% is the looser per-unit uniformity allowance.
The headline: 51.3% of grey-market certs meet the same ±10% bar a pharmacy has to meet, and 68.0% clear the looser ±15% line. The median absolute miss is 9.7%.
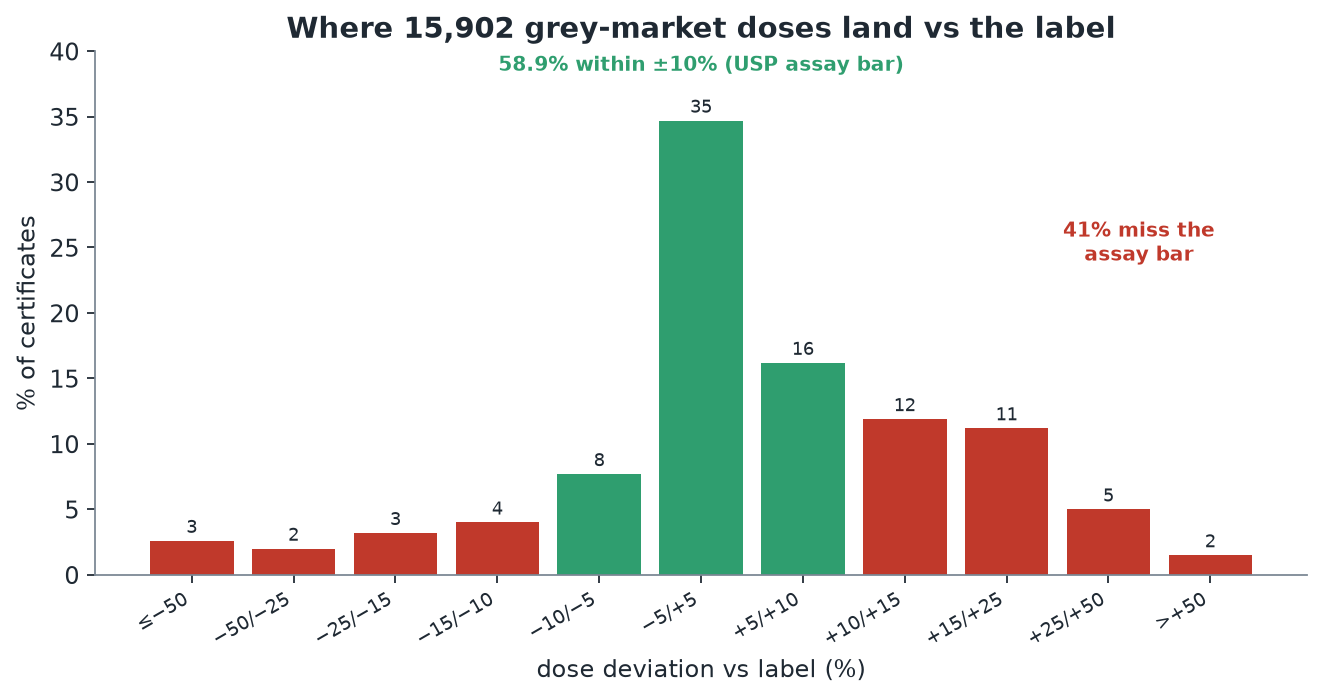
That is a materially worse number than we published in June, and it is worth being straight about why the sentence has changed. In June this section said “the center of the grey market meets pharma’s assay tolerance.” On 15,902 dose-bearing certificates that was 58.9% and the sentence was fair. On 40,271 it is 51.3%, and a coin flip does not deserve the word “meets.” Slightly more than half of grey-market vials clear pharma’s assay bar. Slightly fewer than half do not. The rest of this section stands: the distribution is still centered near label and still skews over rather than under, so the typical vial is not a fraud. But the honest version of the finding is a bare majority, not a comfortable one, and a buyer should read it that way.
Where it falls apart is still the tail. A pharmaceutical lot that came back 40% short would be a recall event with an investigation attached. Here, 680 vials cleared that severity with nobody watching, and the danger is not just the average, it is the variance: a batch that runs from near-empty to over-label cannot be safely dosed at all, because you cannot know which vial you are holding.
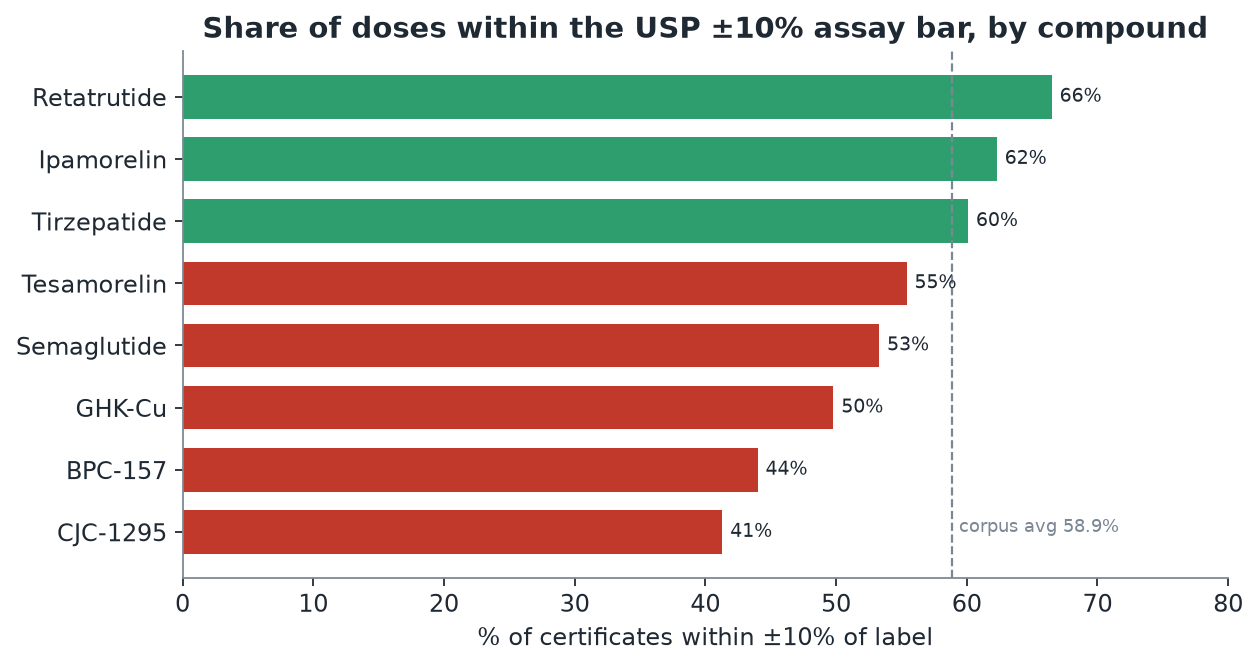
The gap also depends heavily on what you are buying.
Purity: the number everyone screenshots, and the vials with nothing in them
Median grey-market purity is 99.73%, across 50,617 published certificates carrying a purity figure. On paper, that is better than pharma demands. It is also the most misleading number in the entire dataset, for two reasons.
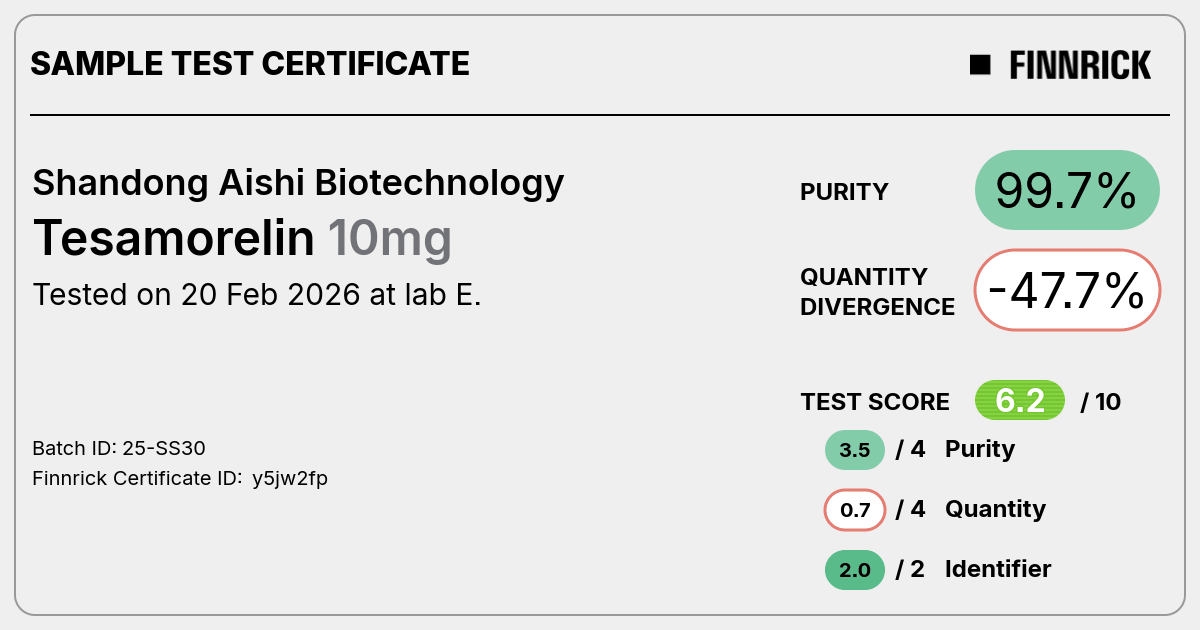
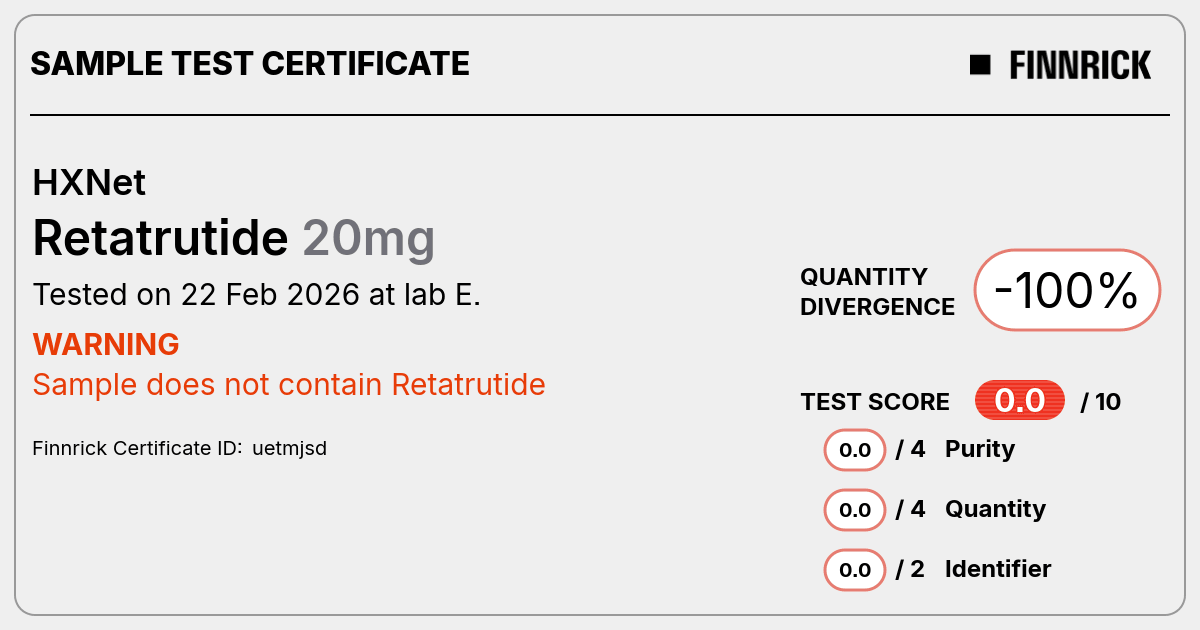
The first reason is that purity is the easy half of the test. A high-performance liquid chromatography assay answers one question well, is this the right molecule and how clean is it, and it is the number every vendor screenshots. It says nothing about how much of that clean molecule is in the vial. The two failures are independent. A vial can be 99% pure retatrutide and still hold a third of the dose. We have the certificate to prove it.
The second reason is the tail again, and here it is not a near-miss, it is a void. 269 certificates, across 95 distinct vendors, reported zero percent of the labeled compound. Not low. None. The “sample does not contain” result, on a product someone paid for and intended to inject.
These zero-content certs are not evenly spread. A handful of vendors are serial: by our count, Peptide Sciences carries 22 of them, Lilipeptide 13, Deuschem 12, Hk Peptides 11. They also concentrate by compound: 30 of the 269 sit on CJC-1295 alone, which is a compound with about 713 purity-bearing certificates in total.
The honest reading of the purity distribution below is not the reassuring mass on the right. It is the red spike on the left.
One of those 269 belongs to a vendor regular readers of this site will recognize. Shanghai ERP Peptide Biotechnology is a high-volume seller with 114 certificates in our corpus, and until June 2026 our own grade gave it an A-plus, because the old score rewarded certificate volume. Two of ERP’s independent certs read 0%, including a retatrutide that contained none of it. That single fact is why our grading now caps any vendor with a zero-content cert. More on that at the end, because this article is also the reason the grade changed.
Endotoxin: the test pharma never skips, and grey market never runs
If you take one thing from this piece, take this one. Dose and purity are quality questions. Endotoxin is a safety question, and it is the question the grey market almost never answers.
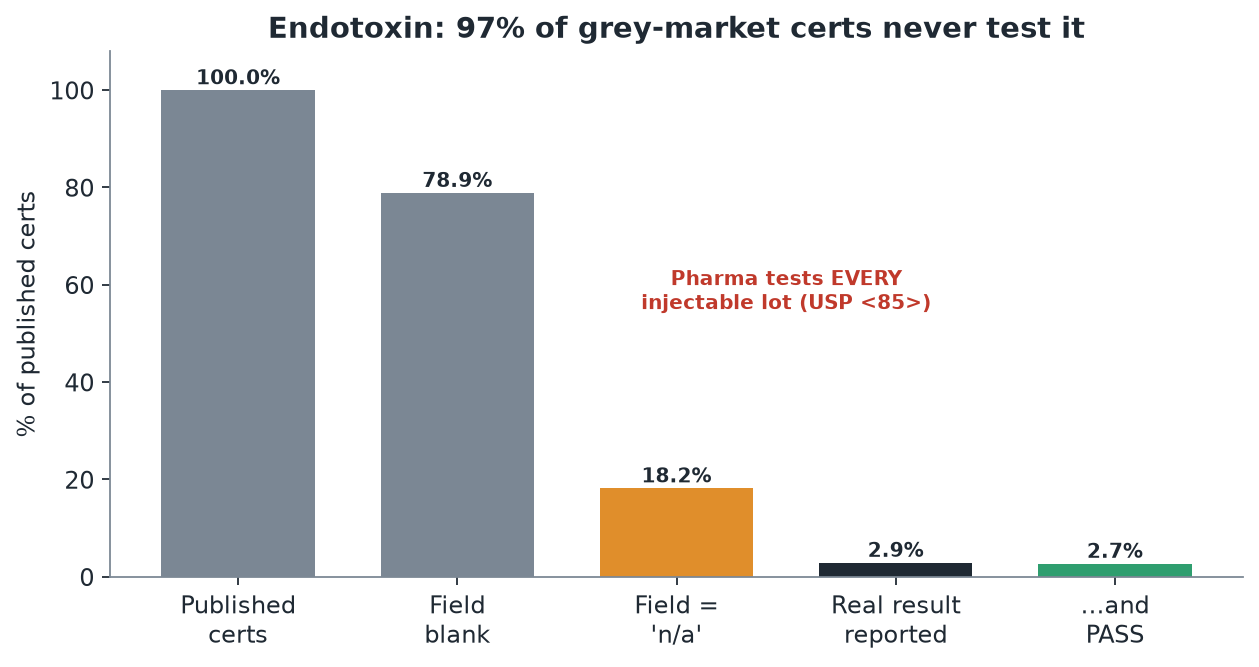
92.5% of certificates in our corpus never test for endotoxin at all. That is an improvement on the 97.1% we published in June, and the improvement is worth naming: the number of certificates carrying a real endotoxin result grew from about 650 to 4,656 in five weeks, roughly a sevenfold rise, while the corpus itself grew less than threefold. More of this market is running the test than was running it in the spring.
The failure rate moved with it, and it moved the other way. Among the 4,656 certificates that report a real result, 53 read fail, detected, or borderline — about 1 in 88, where in June the same method gave about 1 in 15. Do not read that as the market getting safer. The absolute count of failures barely moved; the denominator grew sevenfold underneath it, which is what happens when a testing behaviour spreads from a small set of vendors who had a specific reason to run the assay to a much wider set who now run it as routine. The early sample was adverse-selected. The current one is closer to a real base rate, and a real base rate of roughly one endotoxin failure in ninety injectable vials is still not a number anyone should be relaxed about.
We hold certificates showing NAD-plus vials at hundreds of endotoxin units per vial, against a whole-adult ceiling of roughly 350. A buyer reconstituting that vial and injecting it has no way to know, because for more than nine products in ten the test simply was not run.
This is still the cleanest divide in the dataset, and it is not close. A pharmacy cannot release a single injectable lot without this test. The grey market releases more than nine tenths of its product without it. Sterile is not safe, the test that separates the two survives the autoclave, and it is the test that is missing.
What pharma has that grey market doesn’t: a system
Step back from the individual numbers, because the real gap is structural, and it explains all of them.
A pharmaceutical drug is made under current Good Manufacturing Practice, and 21 CFR 211.165 requires that each batch get “laboratory determination of satisfactory conformance to final specifications, including the identity and strength of each active ingredient, prior to release.” Testing is not a marketing nicety bolted on at the end. It is a legal precondition of selling the lot, and skipping it makes the drug adulterated by statute.
Research-use-only peptides sit entirely outside that structure. They are not approved drugs and not compounded drugs, so they carry none of the guarantees: no required identity, strength, purity, sterility, or endotoxin testing, and no monograph to test against. The “not for human consumption” label is the entire legal shield, and the FDA has now expressly rejected that shield: in a March 31, 2026 warning letter to a peptide seller, the agency wrote that despite “research use only” and “not intended for human consumption” labeling, “evidence obtained from your website establishes that your products are intended to be drugs for human use.” It was one of seven such letters issued that day.
There is one more structural difference, and it is the one we are most implicated in. When the only certificates that reach the public record are the ones a vendor chooses to publish, the public record becomes a marketing surface. A seller can run a hundred tests, post the dozen that pass, and bury the rest, and the aggregate looks immaculate. We documented exactly this mechanism in our XTP investigation, where a vendor with a spotless 99.3% average in our corpus turned out to have shipped 4mg of a labeled 30mg product, with the failing tests living only in private buyer groups. Selective testing is not fraud. It is curation. And curation, at scale, launders trust. The antidote is a corpus that ingests the failing third-party tests alongside the vendor-submitted ones, and refuses to let a vendor be the sole author of its own record.
How this scores every vendor on this site
This article is also the reason our grades changed on June 25, 2026, and the public statement of how they work now.
For a long time our letter grade was, in effect, a count of how many certificates we had scraped for a vendor, dressed up as a quality score. A high-volume seller could carry an A-plus while shipping a zero-content vial, because volume drowned the failures. That is exactly the trust-laundering this piece is about, reproduced in our own math. We fixed it. The grade now rests on the same bars the pharmaceutical industry uses, the ones measured throughout this article:
- Dose fidelity is scored against the ±10% assay bar and the ±15% uniformity bar, not an arbitrary curve.
- Purity is a floor, not a headline, because in this market almost everyone clears 99% and the number does not separate good from bad.
- A critical failure caps the grade. A “sample does not contain” cert, a batch underfilled by 40% or more, a commingled or cherry-picked batch, or an endotoxin failure floors the letter regardless of how many clean certs sit beside it. A vendor that has shipped an empty vial does not get to outrank an honest one on volume.
- Certificate count is shown as confidence, separately, the way a review count sits next to a star rating, never folded into the quality score itself.
Under the old math, Shanghai ERP was an A-plus. Under the new bars, its zero-content retatrutide caps it at C, and the page now says why. That is the only honest version of the grade.
What a buyer should take from this
- Read both halves of the certificate. Purity is the molecule. Quantity is the dose. A vial can be 99% pure and hold a fraction of what you paid for. Always read the fill line against the label.
- Stop treating 99% purity as the finish line. It is the easy half, almost everyone clears it, and it tells you nothing about dose or about what is not on the certificate. The vendors worth trusting are separated by the dose tail and by what they are willing to test.
- Ask the endotoxin question. It is the one test pharma never skips and this market almost never runs. If a vendor selling an injectable cannot show you an endotoxin result, you are the assay.
- Watch the tail, not the average. A 99.3% average with a buried zero-content cert is worse than it looks. The failure a vendor did not want indexed is worth more to you than a hundred passing tests it chose to publish.
- Run any certificate you hold through an independent read. You can OCR and structure any COA, vendor-supplied or your own, with our free COA verify tool, and check it against the corpus before you dose.
- Drill into the compound you actually buy. The averages hide big differences between drugs. See the compound-level dose and purity picture on the retatrutide, tirzepatide, and semaglutide hubs, and the longer arc of vendor failures in the Vendor Graveyard.
Methodology and independence. Regulatory figures are sourced to primary documents: USP <905> and the monograph assay limits, ICH Q3A on impurities, USP <85> on endotoxin, and 21 CFR 211.165 and 21 USC 353a/353b on manufacturing and compounding.
Grey-market figures are computed from 62,079 published certificates in the TitrateLab corpus (Janoshik and Finnrick the largest sources), spanning 2017 to 2026, as of July 31, 2026. Dose figures use the tested-versus-printed-label divergence field and cover the 40,271 certificates that carry one; purity figures cover the 50,617 that carry a purity result; the endotoxin funnel is computed over all 62,079, with a certificate counted as “reporting a real result” when the endotoxin field is neither blank nor “n/a”, and as failing when it reads fail, detected, or borderline. Vendor names attached to specific certs are reproduced from the linked independent reports.
On the numbers moving. This article was first published on June 25, 2026 against a 22,559-certificate corpus. Every corpus figure in it was re-derived on July 31, 2026 against 62,079 and several moved materially, most importantly the ±10% dose share (58.9% to 51.3%) and the endotoxin coverage (2.9% to 7.5%). The June figures reproduce exactly against a June snapshot, so nothing was mis-measured; the corpus grew and the population it describes changed with it. Every superseded figure is listed in the Updates block on this page rather than quietly overwritten. TitrateLab takes no vendor money and sells no placement; see our methodology. If we have a fact wrong, the contact link is in the footer, and we correct the record.