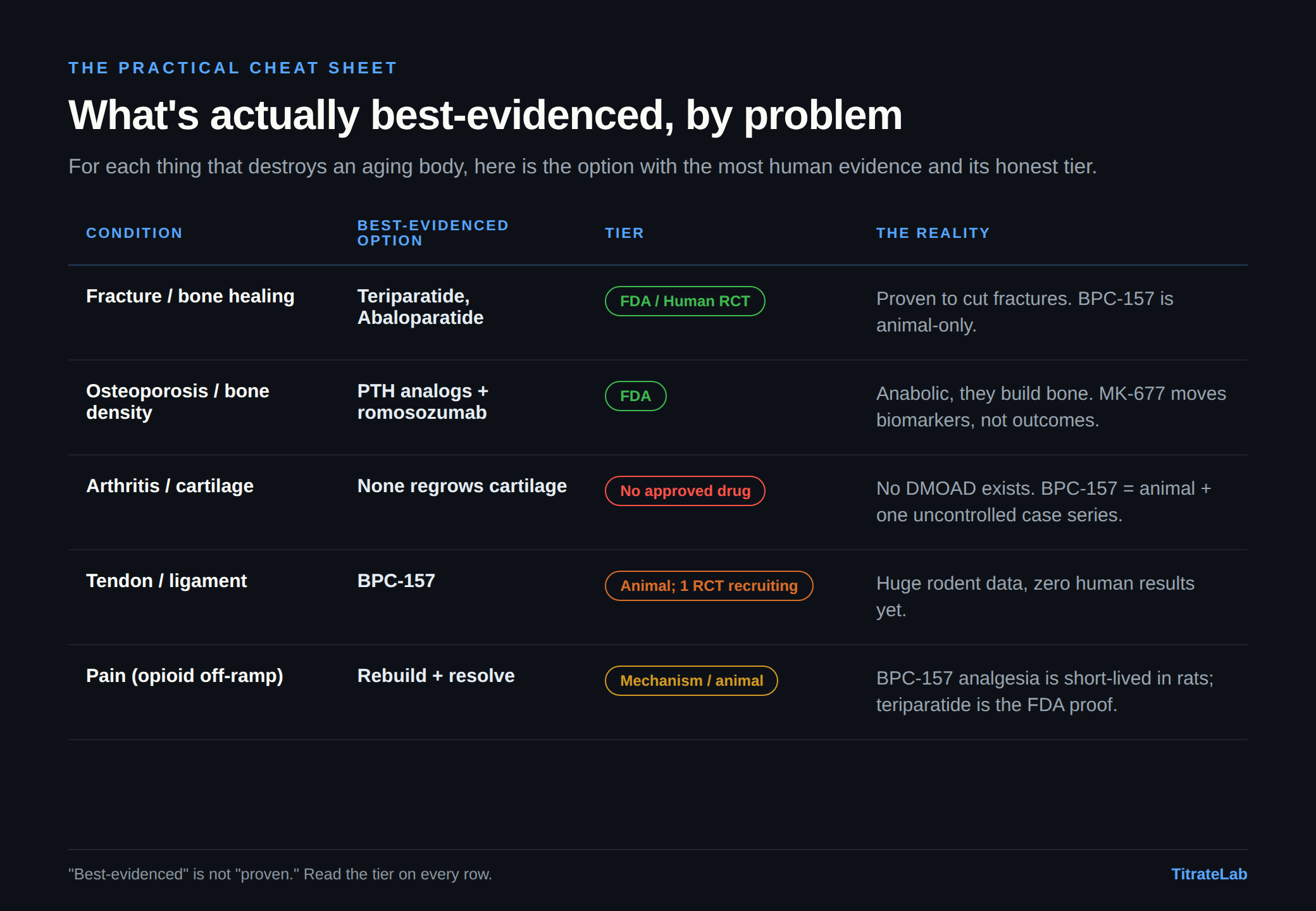
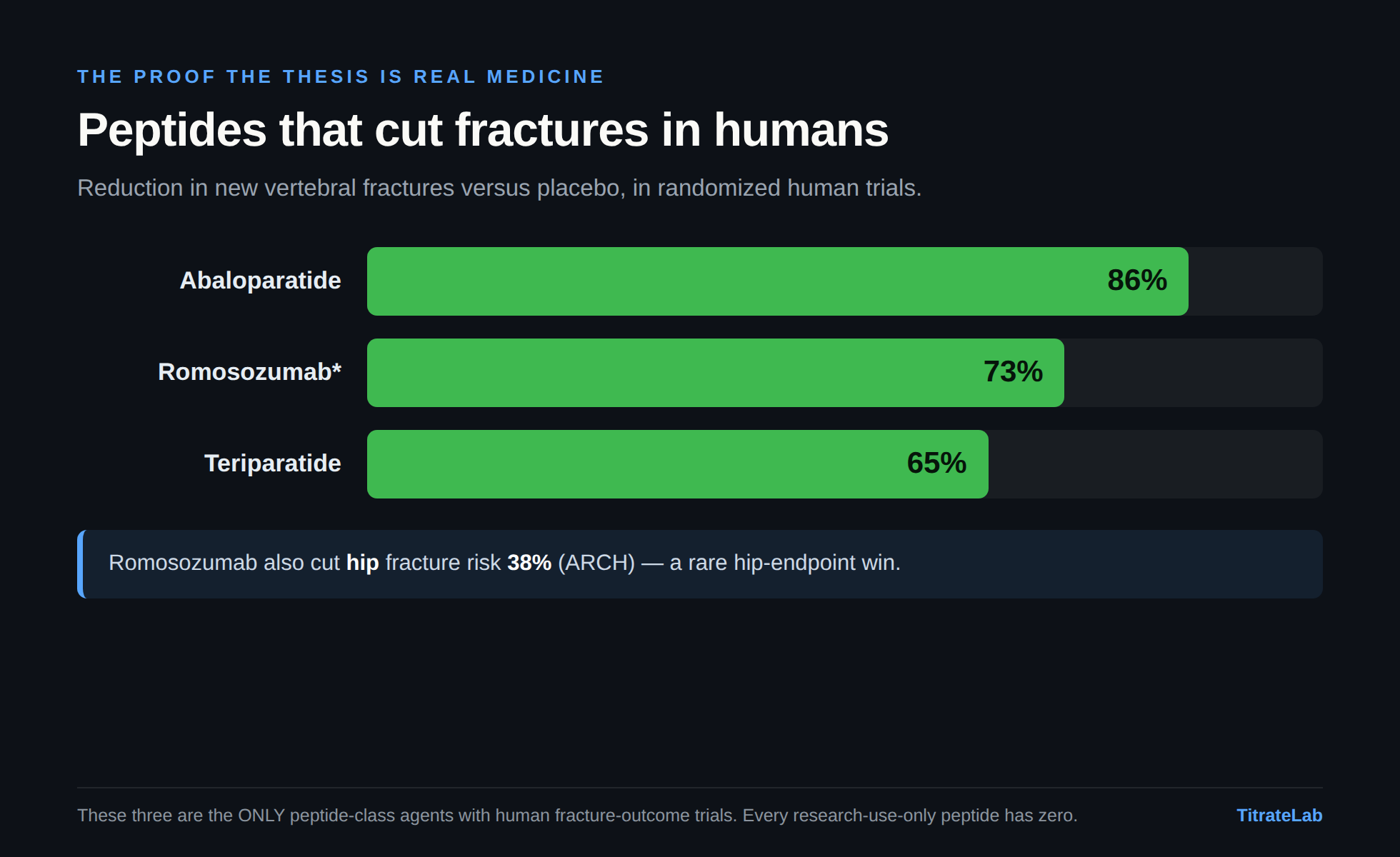
- Building bone is proven medicine. Teriparatide, abaloparatide and romosozumab cut real fractures in human trials (65 to 86 percent). That half of the thesis is FDA-approved fact.
- The joint, tendon and cartilage claims are not proven in people. BPC-157, TB-500 and GHK-Cu have strong, replicated animal evidence but almost no human trials: a real preclinical signal, not yet confirmed in humans.
- No peptide regrows human cartilage or defers a joint replacement. That is the claim furthest ahead of its evidence.
- The most tractable real opportunity is faster fracture healing in the elderly, where the animal evidence is strongest and the endpoint is clean.
- If you inject, the contaminant is often the bigger risk than the molecule. Roughly 30 percent of grey-market peptides have the wrong sequence and 65 percent exceed endotoxin limits. Verify identity and endotoxin first.

FDA-approved anabolic peptides rebuild bone and cut fractures in humans. For the joints, tendons, and nerves the grey market sells hardest, the human cabinet is nearly empty. A tier-by-tier map of what is proven, what is rodent-only, and what is folklore.
TitrateLab research / education. NOT medical advice, NOT a dosing protocol. Every claim below is tiered by evidence strength; an animal or in-vitro result is never allowed to read as human-proven. “Unverified” means the underlying citation could not be confirmed to a primary source.
Tier legend: FDA approved for the stated use | H-RCT human randomized controlled trial | H-obs human observational / case series / pilot (uncontrolled) | Animal animal in-vivo | In-vitro in-vitro / cell culture | Mechanism mechanistic / plausible-only / speculative.
1. The thesis, and why it matters now
The boomer wave is aging into a healthcare system financially and structurally unprepared for it, and the musculoskeletal system is where that collision lands hardest: fragility fractures, osteoporosis, osteoarthritis, torn tendons and ligaments that no longer self-repair, and the chronic pain that rides on all of it. The dominant tools we bring to this are, with few exceptions, symptom management or salvage: NSAIDs and corticosteroids that quiet inflammation without rebuilding anything, opioids that change how the brain reports a damaged joint while leaving the lesion untouched, hyaluronic acid that lubricates a joint it cannot regrow, and, at the end of the line, arthroplasty, the controlled amputation and replacement of a joint that failed.
Our thesis is that we should be far more interested in the other category: interventions that treat the source (rebuild the bone, reorganize the collagen, resolve the inflammation, regenerate the nerve) so that the downstream catastrophe (the fracture, the replacement, the opioid dependency) never happens. The critical move, stated loudly and up front: this thesis is not wishful thinking. It is already proven medicine in one corner of the map (anabolic bone drugs), and almost entirely unproven folklore in the corners the grey market sells hardest (BPC-157, TB-500, GHK-Cu for joints, tendons, and nerves). An honest platform’s entire value is holding those two facts in one hand without letting the first launder credibility onto the second.
A second distinction governs the GH-axis half of this map, and the marketing exists to blur it: replacement-of-a-deficiency is a different evidentiary world from optimization-of-normal-aging. Treating diagnosed adult growth-hormone deficiency, or HIV-associated lipodystrophy, or post-menopausal osteoporosis with a fracture-endpoint-proven drug: that is real disease, real FDA pathway, real benefit. Selling a GH secretagogue to a 62-year-old with a normal-for-age GH axis because “your levels are declining” is a category error. One hypothesis is that the somatopause is adaptive rather than a deficiency. That thread pays off in 3B, where tesamorelin is FDA-approved for one deficiency state and carries zero musculoskeletal-outcome data for healthy aging.
2. The evidence-tier table: where the real leverage actually is
This is the map. Read it first. It is sorted by human leverage, not internet hype; the two run nearly inverse.
| Agent | Class | Best human evidence | Tier | Honest one-line verdict |
|---|---|---|---|---|
| Teriparatide (PTH 1-34) | Anabolic bone peptide | Vertebral fx down 65%, beat risedronate head-to-head | FDA H-RCT | Proven. Regrows bone, cuts fractures. The anchor. |
| Abaloparatide (PTHrP analog) | Anabolic bone peptide | Vertebral fx down ~86% vs placebo (ACTIVE) | FDA H-RCT | Proven. More PTH1R-selective successor. |
| Romosozumab (anti-sclerostin) | Antibody (not a peptide) | Vertebral fx down 73%, hit a hip endpoint (ARCH) | FDA H-RCT | Proven, but a boxed CV warning. |
| Tesamorelin (GHRH analog) | GH-axis peptide | ~15-18% visceral-fat down in HIV lipodystrophy | FDA H-RCT | Approved, but zero musculoskeletal-outcome data. |
| Calcitonin (salmon) | Antiresorptive peptide | Weak/fragile fx signal + a contested malignancy signal | H-RCT (weak) | The cautionary tale: efficacy collapsed under scrutiny. |
| MK-677 / ibutamoren | Oral ghrelin mimetic (non-peptide) | +1.1 kg lean mass / 2 yr; no strength/function/BMD gain | H-RCT | Pharmacology real; outcomes negative; CHF signal in frail (single trial). |
| Thymosin β4 (full-length, RGN) | Repair peptide | Phase 3 eye (1 win/1 fail); Phase 2 wounds safe-but-not-significant | H-RCT (non-MSK) | Real human data, but not in MSK, and not the molecule the market sells. |
| CJC-1295 / ipamorelin / sermorelin | GH-axis peptides | Phase-1 PK only; raises GH/IGF-1 | Mechanism / Phase-1 | No human MSK outcome trial exists, any age. |
| BPC-157 | RUO peptide | One uncontrolled knee case series (n~16); first RCT now recruiting | Animal -> H-obs | Huge rodent corpus, near-empty human cabinet. |
| TB-500 (Tβ4 fragment) | RUO peptide | None: human data is for a different molecule (full Tβ4) | Animal / In-vitro | Don’t conflate with trialed Tβ4. Possibly catabolic in cartilage (correlational). |
| GHK-Cu | Copper tripeptide | Real human topical/skin data; MSK = animal/in-vitro | Animal / In-vitro (topical H-obs) | Deep mechanism, no human bone/joint data. |
| PEDF 29-mer, Link N, B2A, BMP-peptides | Chondrogenic peptides | None (rodent matrix recovery only) | Animal / In-vitro | Genuine rodent cartilage regrowth; human = blank page. |
| KPV / melanocortin fragments | Anti-inflammatory peptides | None in joints (gut models only) | In-vitro / Animal | Plausible anti-inflammatory; joint claims unproven. |
| Resolvins / SPMs | Pro-resolution lipid mediators (not peptides) | Indirect (omega-3 precursor trials) | Animal / In-vitro | Most honest “resolve-the-source” mechanism; mostly preclinical. |
The relative fracture reductions above are not head-to-head except VERO (teriparatide vs risedronate) and ARCH (romosozumab vs alendronate). Baseline risks differed across the placebo-controlled trials, so a larger relative reduction does not always mean more fractures prevented in absolute terms.
The single most important pattern in this table: human-RCT evidence is dense at the bone end (FDA-approved anabolics) and exists at the eye/skin end (full-length Tβ4), and collapses to rodent data exactly at the joint, tendon, cartilage, and nerve targets the thesis cares about most. That gap is the story (Section 4 quantifies exactly how lopsided it is). Anyone selling BPC-157 as a proven tendon or nerve repair, or GHK-Cu as a joint regenerator, is reading rodent data as human data.
The table compresses. Section 3 unpacks each condition in the same descending order, from strongest human evidence to emptiest: bone, then osteoporosis, then cartilage, then tendon, then pain. That order is a deliberate proven-to-unproven gradient.
3. By condition
3A. Fracture and bone healing
This is the corner where the thesis is real, FDA-approved medicine – the anchor for everything else.
The mechanistic key: the Selye paradox Animal/Mechanism, well-replicated. Parathyroid hormone is catabolic to bone when chronically elevated (primary hyperparathyroidism dissolves the skeleton) but anabolic when delivered as a brief once-daily pulse. A spike preferentially wakes osteoblasts before the resorptive machinery spins up. The pharmacokinetics are the mechanism; a long-half-life PTH would destroy bone. This is the conceptual discipline the rest of the field lacks: the waveform is the drug, not “more growth signal.” Any RUO peptide that hand-waves about “growth signaling” with no pharmacokinetic story has not earned the comparison.
The anchor trial H-RCT. Neer et al., NEJM 2001 (PMID 11346808): 1,637 post-menopausal women, teriparatide cut new vertebral fractures 65% and non-vertebral fragility fractures ~53% vs placebo: a fracture endpoint, not a bone-density surrogate. VERO (Kendler, Lancet 2018, PMID 29129436) then beat oral risedronate head-to-head (vertebral fx 5.4% vs 12.0%). Abaloparatide (ACTIVE, Miller, JAMA 2016, PMID 27533157) cut vertebral fractures ~86% vs placebo. Romosozumab, technically a sclerostin antibody rather than a peptide but often considered the state of the art for building bone, cut vertebral fractures 73% (FRAME, PMID 27641143) and, rarely for this field, hit a hip-fracture endpoint (ARCH, PMID 28892457), at the cost of a cardiovascular boxed warning.
Where the RUO peptides actually sit for bone: - BPC-157 Animal: the strongest single result is Sebecic et al. 1999 (Bone, PMID 10071911), a rabbit segmental-defect model where BPC-157 improved bony union comparably to bone grafting. Mechanistically coherent, since callus formation is angiogenesis-dependent and BPC-157’s best-characterized action is VEGFR2-driven angiogenesis (Hsieh 2017), but single-lab, ~25 years old, never independently replicated, zero human fracture data. - TB4/Tβ4 Animal: the best-looking MSK datapoint in the whole Tβ4 corpus is fracture healing in mice (PMID 25042765) with +41% peak force-to-failure and +18-26% mineralized volume. Encouraging biomechanics, in mice. - GHK-Cu Animal, scaffold-delivered: copper is the rate-limiting cofactor for lysyl oxidase (collagen crosslinking) and drives angio-osteogenic coupling; the load-bearing result (copper-peptide silk scaffold, Chem Eng J 2021) is M2-macrophage polarization plus neovascularized bone regeneration, but as an implanted construct coating, not a systemic drug.
Realistic potential. The highest-leverage, most-tractable RUO human hypothesis in this report is acute fracture-union acceleration in the elderly, where shaving two weeks off time-to-union meaningfully cuts immobility-driven mortality. It matches the rodent evidence base; it has a clean objective endpoint (radiographic time-to-union); and it is exactly the trial nobody has run.
Honest verdict for bone: the anabolic-drug destination is proven and reachable FDA/H-RCT; the RUO peptides have a plausible on-ramp and an empty human cabinet Animal. The tractable human bet is acute fracture-union acceleration, not bone-density optimization.
3B. Osteoporosis / bone density
The clean lesson here is the BMD-vs-fracture gap, taught by MK-677. MK-677 (ibutamoren, an oral ghrelin mimetic, non-peptide, but the center of gravity of the “GH-axis peptide” conversation) has the only multi-year human MSK RCT data in its class, and the results are a masterclass in why biomarkers lie: - Svensson 1998 and Murphy 1999 H-RCT: MK-677 raises bone-turnover markers, but on both sides (formation and resorption), i.e. faster remodeling, not net accrual. - Murphy 2001 H-RCT, the pivotal negative: in osteoporotic post-menopausal women, MK-677 monotherapy did not significantly increase BMD at any site. The antiresorptive (alendronate) is what moved density. - Nass 2008 H-RCT (PMID 18981485), the flagship 2-year trial: GH/IGF-1 restored to young-adult range, fat-free mass +1.1 kg, but verbatim, “increased fat-free mass did not result in changes in strength or function,” plus rising fasting glucose and reduced insulin sensitivity. - Adunsky 2011 H-RCT (PMID 21067829), the trial nobody quotes: in elderly hip-fracture patients, the exact thesis population, most functional endpoints were null and this single trial was stopped early for a congestive-heart-failure signal (6.5% vs 1.7%).
The reference ceiling H-RCT: even recombinant GH itself, in the Liu 2007 Ann Intern Med systematic review (31 RCTs), moved body composition (~2 kg fat down, ~2 kg lean up) but produced no consistent strength or functional gain and more edema, arthralgia, carpal tunnel, and glucose intolerance. The secretagogues cannot plausibly beat the drug they mimic, and that drug already failed its outcome test in healthy aging.
The Tβ4 osteoporosis whisper In-vitro: in periodontal ligament cells Tβ4 suppressed osteoclastogenesis, an anti-resorptive signal that, paired with the mouse fracture biomechanics, hints at a “build plus spare” profile. In-vitro only.
Honest verdict for osteoporosis: the GH/IGF-1 axis reliably moves DEXA numbers and turnover markers and reliably fails to move strength, function, density-as-monotherapy, or fractures, and the one frail-elderly trial showed cardiac harm. The proven path is the anabolic-bone class. The GH-axis field has been stuck at “interesting biomarkers” for 25 years for a reason that is not biology: MK-677 is off-patent/abandoned and the peptide analogs are unpatentable, so no one will ever fund the outcome trial.
3C. Arthritis and cartilage: the hardest target in the body
Frame this brutally up front. Hyaline cartilage is avascular, aneural, and alymphatic; mature chondrocytes are post-mitotic. OA is a one-way street, which is why the entire standard of care is symptom management and there is no FDA-approved disease-modifying OA drug (DMOAD) that regrows cartilage. The honest benchmark: even the best-studied biologic DMOAD candidate, sprifermin (rhFGF-18), in the rigorous FORWARD Phase 2 RCT, produced a real but sub-millimeter (~0.05 mm) cartilage-thickness gain with no clear symptom benefit outside a high-risk subgroup. If the gold-standard injected growth factor barely moves structure, read every grey-market peptide claim against it.
BPC-157 Animal + H-obs: rat OA (ACL+MCL transection+meniscectomy) showed near-normal articular surface at 4 weeks, but the load-bearing source is a 2014 FASEB meeting abstract, not a peer-reviewed paper. The human data is one uncontrolled retrospective intra-articular knee case series (Lee, PMID 34324435, n~12-17, ~91% reporting relief). An uncontrolled, unblinded intra-articular injection series cannot be separated from the large, well-documented placebo response that intra-articular injection of even saline produces in knee OA, which is exactly why the blinded NCT07437547 trial matters. Hypothesis-generating only.
TB-500 / Tβ4, the “read the direction of effect” cautionary case In-vitro/H-obs: in chondrocytes Tβ4 increased pro-MMP-9 (a catabolic, matrix-degrading enzyme, PMID 12440937), and serum/synovial Tβ4 is elevated in worse knee OA. This is correlational: damaged cartilage may upregulate Tβ4 as a repair response, so the direction of causation is unproven. Still, this is why “tissue healing” claims do not transfer from tendon and wound contexts to cartilage: Tβ4 for cartilage is not supported as regenerative and may be net-catabolic.
GHK-Cu In-vitro/inferential: drives the collagen/GAG/decorin program and balances MMP/TIMP in fibroblasts and wounds, mechanistically attractive for slowing OA catabolism, but a load-bearing primary chondrocyte paper could not be verified, and there is no GHK-Cu in-vivo OA model and no human OA trial. The OA claims circulating online trace to content-farm sites with no primary citations; do not treat as evidence.
The genuinely interesting chondrogenic frontier Animal/In-vitro (mapped by Liao, Cartilage 2024, PMC11556548, whose own conclusion is that in-vivo evidence is “currently insufficient”): - PEDF 29-mer + hyaluronic acid Animal, the strongest recent regeneration-specific result: in rat MIA-OA, intra-articular PEDF 29-mer induced chondrocyte regeneration and matrix recovery in the model via PEDFR->STAT3 (peer-reviewed, Bone Joint Res 2024, PMID 38555936). Rat-only. - Link N Animal, endogenous link-protein fragment, binds BMPR-II->BMP-7/Smad1/5->Sox9/aggrecan/Col-II, plus IL-1β suppression plus analgesia within 6 hours (independent of structural repair). Dual anabolic plus anti-catabolic plus analgesic, but its disc-repair effect is species-specific, and there are no human joint trials. - B2A, BMP-2 peptide, GFOGER, RGD, WYRGRL (cartilage-homing tag), cationic aggrecan-binders, mostly in-vitro scaffold/tissue-engineering tools, not injectable drugs.
KPV / melanocortin fragments In-vitro/Animal: the α-MSH C-terminal tripeptide suppresses NF-κB/MAPK->TNF-α/IL-1β/IL-6, but its real efficacy data are in gut models, not joints. Worth noting that the melanocortin axis is a real druggable arthritis target (AP1189/resomelagon hit ACR20 60.6% in a Phase 2a RA trial), but AP1189 is an oral small molecule, not a peptide, and it is RA (autoimmune), not OA. It lends mechanistic, not clinical, plausibility to the peptide fragments.
The “save a hip/knee replacement” question, answered honestly: for end-stage, bone-on-bone OA (Kellgren-Lawrence 4), there is no credible evidence any peptide defers arthroplasty. The chondral substrate to rebuild is gone, and these agents need viable chondrocytes/progenitors to act on. The only plausible (hypothesis-grade) niche is early-to-moderate OA (KL 1-2), slowing catabolism and nudging endogenous repair. Anyone marketing peptides as a replacement for arthroplasty is miles ahead of the evidence.
3D. Tendon and ligament: the deepest rodent corpus, the emptiest human one
This is BPC-157’s reputational home ground, and it is entirely Animal/In-vitro.
Mechanism In-vitro: Chang 2011 (PMID 21030672), BPC-157 drives FAK-paxillin phosphorylation in tendon fibroblasts (true pathway activation, not just expression) -> dose-dependent migration, survival under oxidative stress, explant outgrowth. Chang 2014 (PMID 25415472), upregulates the GH receptor in tendon fibroblasts, sensitizing tissue to the body’s own GH – a lower-risk mechanism than adding exogenous growth factor, if it holds in vivo, which is unshown in humans.
In-vivo Animal: Achilles transection healing (Staresinic 2003, PMID 14554208); MCL transection (Cerovecki 2010, PMID 20225319) with higher load-to-failure, a real biomechanical endpoint, effective by IP, oral, and topical routes carrier-free; muscle crush/transection healing. The rodent consistency across injury types and routes is consistent and reproducible Animal, and unproven in humans.
Tβ4 Animal: rat MCL healing and tendon collagen reorganization (uniform, larger-diameter fibrils vs disorganized controls), mechanistically apt (actin-driven migration plus anti-fibrotic collagen organization), human-unproven.
The reputational honesty check Mechanism: BPC-157’s online reputation comes from the breadth of positive rodent models, not from any human regeneration proof. “Heals a transected rat Achilles in weeks” has been amplified online into “heals human tendons fast,” which is not demonstrated. The reputation runs ~20 years ahead of the human evidence.
The one bright spot [H-RCT, in progress]: NCT07437547, the first rigorous test, a Phase 2 randomized, double-blind, placebo-controlled trial of subcutaneous BPC-157 for acute grade-II hamstring strain, co-primaries return-to-sport time plus MRI injury-volume change. Results ~2027. Until then, every confident tendon claim is rodent extrapolation. GHK-Cu for tendon/ligament is total white space, no study at all, despite driving exactly the collagen/decorin/LOX-crosslinking program tendon repair needs.
Honest verdict for tendon and ligament: the deepest, most consistent rodent corpus in the report Animal, against a near-total human void. One Phase 2 RCT will decide whether any of it transfers; until those results land, every tendon claim is rodent extrapolation.
3E. Pain at the source: the opioid off-ramp
The mechanistic divide is the whole point. Opioids change how the brain reports a damaged joint; they do nothing to the inflamed synovium, the torn tendon, or the demyelinated nerve. Worse, chronic mu-opioid agonism actively degrades itself: tolerance plus opioid-induced hyperalgesia (MOR->BDNF->KCC2 downregulation->chloride dysequilibrium that amplifies pain; up to ~30% of chronic users), a therapy whose efficacy decays while its lethality climbs. Close to a worst-case analgesic for a fragile, polypharmacy-laden aging population.
“Addressing the source” means hitting one of three targets: resolve inflammation, rebuild matrix, or regenerate nerve. The peptide map:
- The FDA-grade proof of concept FDA/H-RCT: teriparatide/abaloparatide are peptides that rebuild tissue at the source and cut the downstream catastrophe (fractures) in rigorous RCTs. Proof the thesis is achievable.
- BPC-157 nerve/analgesia Animal/Mechanism: sciatic-nerve regeneration (Gjurasin 2010, PMID 19903499), abolished autotomy behavior, spinal-cord-injury functional recovery (PMC6604284). But the sobering part comes from BPC-157’s own analgesia review (PMC13026520): in incisional/formalin rat models the antinociception diminished by ~7 days and acted only in the early inflammatory phase. The authors conclude it is a short-lived peripheral anti-inflammatory effect, NOT a centrally mediated or healing-driven analgesic. It has no known opioid-receptor mechanism and no abuse/dependence liability, a genuinely attractive frame, but it is human-unproven.
- The pro-resolution class, resolvins / SPMs Animal/In-vitro: the most mechanistically honest answer to “resolve the source of pain.” These lipid mediators (from EPA/DHA, technically not peptides, flagged honestly) don’t block inflammation, they switch it off: desensitize TRPV1/TRPA1 nociceptors, drive macrophage efferocytosis, damp central plus peripheral sensitization. “Failed resolution = chronic pain” is now a leading paradigm. Human data is limited to omega-3 precursor trials; synthetic analogs are preclinical.
The honest off-ramp verdict: opioids act in minutes; regeneration takes weeks-to-months. Any real off-ramp is a bridge (taper as tissue heals), not a swap. The entire regenerative stack is currently supported by animal data, mechanism, and one case series. A compelling, well-grounded hypothesis; not a protocol to run today.
4. The hard truths

The human-trial desert. For the RUO frontier the evidence is lopsided past parody. The 2025 HSS Journal systematic review of BPC-157 (PMID 40756949) screened 544 articles and found exactly one clinical study: 35 of 36 were animal. That ratio is the field. BPC-157’s entire human corpus is three uncontrolled pilots from a single Florida group (Lee: knee n~16, interstitial cystitis n=12, IV PK n=2), a cancelled Phase 1 (NCT02637284), and one RCT now recruiting. BPC-157 also has no identified receptor after 25 years, and near-universal positive findings concentrated in one lab (Sikiric, Zagreb). The single-lab problem is the real weakness; “no known receptor” is a softer one (lithium and metformin went decades the same way), and like MK-677’s gap it may reflect structural underfunding rather than failed biology. CJC-1295/ipamorelin/sermorelin have no human MSK outcome trial at any age. GHK-Cu’s real human data is topical/cosmetic skin. TB-500 has zero human data of its own: every legitimate Tβ4 trial used full-length 43-aa Tβ4 (RGN-352/259/137), a chemically different molecule from the grey-market Ac-LKKTETQ fragment; a vial sold as “TB-500” may contain the fragment, full Tβ4, a mix, or neither.
Lean mass is not strength, and neither is fracture protection. The cross-cutting law behind 3B’s rhGH and MK-677 data: the DEXA number moves; the muscle you can actually use and the fractures you actually avoid do not follow. Strength is neuromuscular, not just mass; the axis grows tissue it cannot innervate or load into useful force.
BMD is not fracture; surrogate is not outcome. Even FDA-approved bone anabolics only work as a managed multi-phase protocol: “build, then protect.” The anabolic window is finite (~6-12 months); gains are lost if not locked in with a follow-on antiresorptive (ACTIVExtend, PMID 29800372; FRAME/ARCH demonstrate this prospectively), and sequence direction matters (denosumab->teriparatide is actively harmful short-term). Any serious regenerative thesis inherits this protocol discipline: a peptide that builds tissue you then fail to retain did nothing.
The IGF-1 / cancer plus tumor-angiogenesis concern, take it seriously, in exactly this population. Every “build tissue / grow vessels” peptide is by definition pro-angiogenic and pro-proliferative: the same axis tumors exploit. Higher circulating IGF-1 is associated with modestly higher prostate-cancer risk in human meta-analysis (Travis/EHPCCG 2016). BPC-157’s VEGFR2 mechanism and Tβ4’s correlation with tumor invasiveness are coherent theoretical concerns. None is a demonstrated human harm. But no RUO peptide trial is long or large enough to detect a cancer-incidence effect, so “no harm shown” here means “not looked for.” This matters most precisely because the thesis population, the aging, has the highest baseline prevalence of occult neoplasia. The right reading is unquantified caution – not panic, not dismissal.
The osteosarcoma teaching case (cuts both ways). Teriparatide carried an osteosarcoma boxed warning for ~18 years based on Fischer-344 rats dosed at 3-60x human exposure for roughly 80% of their lifespan: a species artifact. ~18 years of structured human pharmacovigilance found no excess, and the FDA removed the warning and the 2-year cap in 2020. The lesson: (a) a scary rodent signal can be a species artifact human data overturns; don’t let animal results masquerade as human truth; but (b) we can only say “it’s fine in humans” because someone ran a two-decade mandatory surveillance program. The grey-market peptides have neither the RCTs nor the pharmacovigilance; they have only the rat, with no path to step (b).
The regulatory reality (as of mid-2026, and time-sensitive). Almost everything here except teriparatide, abaloparatide, romosozumab, and tesamorelin is research-use-only / not FDA-approved for these uses. BPC-157 was placed in FDA 503A Category 2 (significant safety risk) in 2023 and removed from Category 2 effective April 22, 2026, but removal from Category 2 is not approval and does not add it to the positive bulks list; it remains investigational, and is one of seven peptides (BPC-157, KPV, TB-500, MOTS-C, DSIP, Semax, Epitalon) under PCAC 503A review (July 23-24, 2026). BPC-157, TB-500, and MK-677 are WADA-banned. FDA explicitly flagged compounded injectable GHK-Cu for immunogenicity/aggregation risk.
The grey-market supply risk, the most concrete present danger. Independent analyses found roughly 30% of online peptides had the wrong amino-acid sequence and roughly 65% exceeded endotoxin safety thresholds (sampling frames and assays vary across these analyses, so treat the figures as indicative rather than precise); heavy metals, truncated sequences, residual solvents, and microbial contamination are documented. For an injected, and especially an intra-articular, product, the contaminant is frequently a bigger acute risk than the peptide itself: a joint is a closed, poorly-vascularized space, and a contaminated injection there can mean septic arthritis. This is squarely TitrateLab’s COA wheelhouse: purity/endotoxin/identity verification is the load-bearing safety layer, not an afterthought.
5. The ambitious frontier (clearly labeled speculation, Mechanism, a research agenda, not claims or advice)
Local/sustained delivery is the real unlock, not new payloads. The most evidence-grounded frontier idea: concentrate the regenerative signal at the lesion and keep it out of systemic circulation (which also blunts the tumor-angiogenesis worry). Concrete bets: BPC-157 or PEDF-29mer in a resorbable scaffold/fibrin glue at a surgical tendon-to-bone repair (leveraging BPC-157’s demonstrated carrier-free local activity); Tβ4-loaded hydrogels/sutures intra-callus; GHK-Cu as a release-tuned eluting coating on a titanium orthopedic/dental implant for osseointegration in osteoporotic/diabetic bone; a cartilage-homing tag (WYRGRL or the cationic aggrecan-binder) fused to an anabolic payload so one intra-articular dose dwells in cartilage for weeks instead of clearing in hours. Two of those three building blocks already have rodent in-vivo support; the combination is untested.
Rational combinations (untested, compounds the unknown-safety problem). The thesis-coherent stack maps the three targets: resolve (SPM/resolvin analog to switch off the neuro-immune amplifier) plus rebuild (GHK-Cu for matrix/copper/LOX, or Tβ4 for migration) plus regenerate nerve (BPC-157’s rodent NGF/myelination signal) plus anchor the bone bed (PTH-analog where subchondral/osteoporotic bone is the failure point). The popular BPC-157+TB-500 pairing is mechanistically complementary on paper (angiogenesis/FAK-migration plus actin-driven motility) with zero controlled head-to-head data. For bone, the most defensible untested experiment is GH-secretagogue + a modern antiresorptive/anti-sclerostin + progressive resistance loading: let IGF-1 drive osteoblasts while you clamp resorption and supply the mechanical stimulus that converts mass into usable strength (the part the “drug alone fixes the boomer” framing most cleanly refutes).
The trials it would actually take. To convert thesis into medicine: (1) finish BPC-157’s hamstring RCT (NCT07437547), then a properly powered, blinded, placebo-controlled intra-articular knee-OA RCT with both a pain/function endpoint (WOMAC/KOOS) and a structural MRI cartilage readout, in early OA (KL 1-2) where substrate still exists, on the FORWARD/sprifermin template, at least 2 years, and honesty that even “success” likely looks like sub-millimeter structural gain plus slowed progression, not a regrown joint; (2) a real Phase I PK/safety with dose-escalation and anti-drug-antibody monitoring, run by independent investigators to break the single-lab/single-group pattern; (3) dose-ranging SPM/resolvin human chronic-MSK-pain RCTs with pharmacodynamic blood levels, the most mechanistically honest “treat-the-source-of-pain” shot; (4) the decisive study the field lacks, an opioid-taper RCT (standard care vs standard care + regenerative-peptide stack), with opioid morphine-milligram-equivalents and function as co-primaries; (5) carcinogenicity/long-term safety given the angiogenesis mechanism and aging target. Every arm must use COA-verified, endotoxin-screened, sequence-confirmed peptide, the single biggest reason past “results” are uninterpretable.
6. What an honest, mission-driven platform should do with this
-
Never launder the bone evidence onto the RUO frontier. The same page that celebrates teriparatide’s 65% fracture reduction must state, in the same breath, that BPC-157 has one uncontrolled case series and TB-500 has zero human data of its own. The tier label is the product. Strip it and you become exactly the content-farm/vendor copy this report exists to refute.
-
Make purity the headline safety layer, not a footnote. For injected and intra-articular peptides the contaminant often outranks the molecule as the acute hazard. A platform whose COA corpus reproduces the same ~30% wrong-sequence and ~65% endotoxin-breach picture from Section 4 has a load-bearing, differentiated, true safety contribution: verify identity, endotoxin, and fill before anyone discusses mechanism.
-
Lead with the honest gap, not the rodent hope. The most defensible, mission-aligned framing is: the regenerative thesis is biologically sound and partially proven (PTH-analogs, FDA, fractures), mechanistically alive and rodent-validated for the frontier (PEDF-29mer, Link N, BPC-157, Tβ4), and the human-RCT cabinet for the frontier is near-empty. That is not a hedge. It is the most useful thing a reader can be told.
-
Point at the tractable wins, not the over-promises. The defensible near-term contributions are (a) rigorous human safety/PK data for the most promising candidates, (b) intra-articular and scaffold delivery engineering, and (c) affordable access to the medicine that already works, not more rodent efficacy papers, of which there are already plenty. On access: branded teriparatide runs roughly $4,000 to $5,100 per 28-day pen, abaloparatide $30k to $50k/yr, romosozumab $21k to $24k/course (these are list prices, not a cost ranking; the teriparatide pen annualizes to more than the abaloparatide figure). Biosimilar teriparatide is the proof-of-concept that an effective bone anabolic can get cheap, and the benchmark the RUO frontier would have to beat on access without sacrificing the evidence base. Arthritis reversal and replacement-avoidance are where the evidence is thinnest; acute fracture-union and post-surgical soft-tissue augmentation are where it is strongest. An ambitious platform aims its credibility at the second, not the first.
The smooth-landing vision. The honest version is not “peptides replace joint replacement.” It is a stratified, source-treating layer that delays the catastrophe: anabolic bone protocols (already real) cut the fragility-fracture wave; localized regenerative delivery augments surgical and acute soft-tissue repair in the elderly so injuries heal faster with less immobility-driven mortality; early-OA intervention slows the one-way street before the substrate is gone; and a pro-resolution plus rebuild bridge tapers opioids as tissue heals rather than substituting one receptor-blocker for another.
Bottom line. The thesis (build the tissue, don’t mask the pain or amputate the joint) is real medicine at the bone-anabolic end and a compelling, well-grounded hypothesis with a near-empty human cabinet everywhere else. The honest, genuinely ambitious move is to pursue the frontier as a research program (COA-verified material, independent investigators, objective endpoints, localized delivery) while telling every reader, every time, exactly which tier the claim in front of them lives on.
Research/education only, not medical advice, not a dosing protocol. Citation notes: the Miller/ACTIVE abaloparatide trial is PMID 27533157 (an earlier draft cited a wrong PMID); the 2025 BPC-157 systematic review (PMID 40756949) was published in HSS Journal, not the American Journal of Sports Medicine. The following remain flagged for confirmation before publication: the BPC-157 rat-OA result (conference abstract only), the GHK-Cu primary chondrocyte source (could not be verified; published GHK-Cu matrix data are in fibroblast/wound models, not chondrocytes), and several content-farm GHK-Cu/wound figures. Regulatory status (FDA 503A Category-2 removal, the PCAC 503A review, and the named NCT numbers) is current as of mid-2026 and is inherently time-sensitive; re-verify and date-stamp before republication. Secondary preclinical PMIDs cited in Section 3 (Sebecic 10071911, Cerovecki 20225319, Chang 21030672 / 25415472, Gjurasin 19903499, the mouse fracture 25042765, the Tβ4 pro-MMP-9 12440937, the Lee knee case series 34324435) were outside the verified citation set and should be confirmed independently.